
Accelerated Resolution Therapy (ART): what it is, where it came from, and how to know if it fits
Accelerated Resolution Therapy (ART) is a structured trauma therapy that uses guided eye movements and imagery-based protocols to help distressing memories stop lighting up the nervous system like the threat is happening right now.

Most people end up here because they’re tired of a memory, trigger, or body reaction taking over their day. And a lot of trauma therapists end up here because they want reprocessing to be contained, paced, and clear, not a vague “let’s talk about it until it shifts.”
This post is for the real-life questions that come up after the definition: where ART came from, what it can look like in session (high level), what it tends to be best for, and how I think about readiness, dissociation, and fit.
What Is ART ?
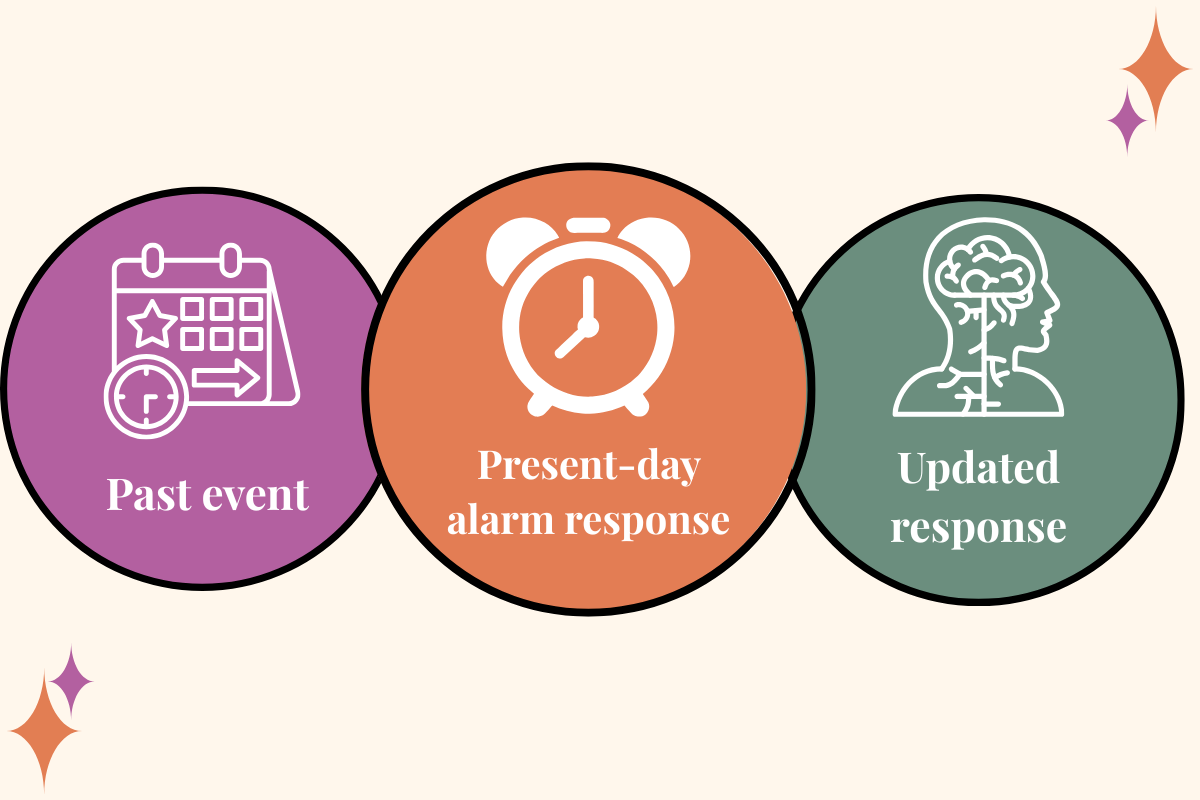
When I talk about ART, I’m talking about a specific goal: helping the brain and body respond to a memory as a past event instead of a current threat.
A lot of clients can explain their trauma clearly and still have their body react as if it’s happening now. That isn’t because they’re not trying hard enough. It’s because trauma isn’t only stored as a story. It can show up as sensation, image, and threat-response patterns that fire automatically.
ART is designed to work directly with that stuck “here and now” response, especially when the target is clear and specific.
One scope note: I’m not ART-trained, so I’m not teaching protocol here. This is education and orientation meant to support good clinical decision-making and informed choice.
Where ART came from

ART was developed in 2008 by Laney Rosenzweig, an EMDR-trained clinician. You’ll often hear that ART was developed out of EMDR, and that’s a useful shorthand as long as it doesn’t turn into “so it’s basically the same thing.”
They share some visible elements (like eye movements), but ART is its own approach with its own structure and protocols. If you’re a therapist, this matters because informed consent gets muddy when we talk like models are interchangeable. If you’re a client, it matters because what it feels like in the room can differ based on the model and the clinician’s pacing.
What an ART session can look like
One of the biggest sources of confusion about ART is that people hear “eye movements” and assume they already know what the session will look like, or they assume it will feel exactly like EMDR. Even when models share a visible element, the experience can be different depending on the structure, the pacing, and how imagery is used.
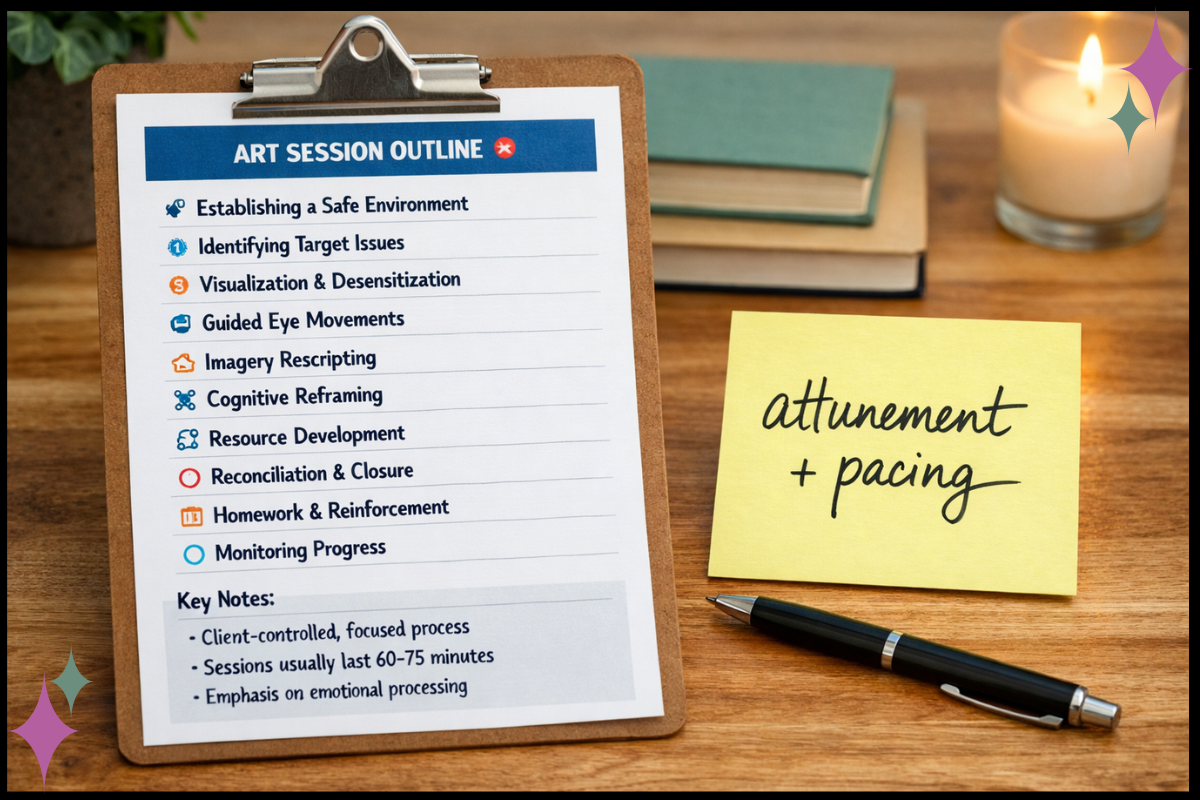
Here’s a high-level picture of what often happens in ART, without turning this into training.

You identify a target.
Not your entire history. Usually something specific: a memory, an image, a moment, or a trigger that reliably spikes distress.You notice the current response.
What happens in the body? What emotions show up? What does your mind conclude about you or the world when that target is activated?You do guided sets of eye movements.
The therapist guides the eye movements while tracking activation and pacing.Imagery-based work is used to support updating.
This is a distinguishing feature people often associate with ART: imagery is used in a structured way to help the brain “file” the memory differently, so it stops hitting with the same charge.
What I want you to hear most clearly is this: a good ART session is not a performance of speed. It’s a practice of pacing, consent, and nervous system tracking. The structure is there to support safety, not override it.
Why ART can be efficient (without turning it into a miracle story)
ART has a reputation for helping people make meaningful progress in fewer sessions, especially when the target is clear and discrete.
That can be true. It can also get oversold.

Here’s how I think about it clinically: when a target is clean (a specific moment, image, or belief that keeps looping) and the person has enough stability to stay present, the nervous system can update quickly. Sometimes the shift is immediate enough that clients feel surprised by their own relief.
But when the target is layered (developmental trauma, attachment injury, ongoing stress, high dissociation, multiple competing triggers), pushing “efficiency” can backfire. Not because the model is bad, but because the pace is mismatched to the person’s nervous system. That’s how people end up flooded, shut down, or feeling worse after session.
So I don’t chase speed. I look for effective change that holds over time, with enough support and integration built around it.
ART misconceptions that come up a lot
1) “Is ART just EMDR?”
No, but I understand why people ask.
From the outside, both can involve a client bringing a target to mind while doing guided eye movements. And yes, ART has EMDR roots because the developer was EMDR-trained. That’s the overlap people see.
Where the confusion starts is when we treat “uses eye movements” like it’s the whole model. It isn’t. Eye movements are one ingredient. The model is the recipe.
Plain-language version: EMDR and ART are related approaches in the trauma reprocessing family, but they aren’t interchangeable. They use different structures, different protocols, and often a different “feel” in the room.
If you’re a client, it’s fair to ask:
“Are you trained in ART specifically?”
“What does ART look like in your hands?”
“How do you decide whether we’re doing ART versus another form of reprocessing?”
If you’re a therapist, the clinical piece I don’t want us to gloss over is informed consent. When we say “it’s basically EMDR,” clients can walk in with expectations that don’t match what we’re actually doing. Clarity reduces fear and makes pacing easier.
2) “Will ART erase my memory?”
No. ART isn’t about deleting what happened or making you forget your story.
The goal is to reduce the charge and the present-day reaction so the memory becomes something you can remember without your body responding like you’re back in it.
A lot of people get nervous about imagery work because it can sound like rewriting history. That’s not the goal. The goal is helping the brain and body stop reliving the experience as an active threat. You keep the facts. The alarm response doesn’t run the show anymore.
3) “If it can be fast, does that mean it’s shallow?”
Not automatically.
Some changes are quick because the nervous system finally gets the update it needed. Other work needs time because the target is layered, because life is currently chaotic, or because the person needs more stabilization before reprocessing is a good idea.
Depth isn’t measured by session count. Speed isn’t proof of anything on its own. I look for: Is the pace matched to this person? Does the change stick? Can they integrate it?
4) “Is ART safe for everyone?”
No trauma reprocessing model is a fit for everyone at every time.
Safety depends on readiness, stability, pacing, consent, and the clinician’s skill with nervous system tracking. A method doesn’t create safety by itself. The way it’s done creates safety.
And this is also where dissociation matters, so let’s talk about that directly.
Fit and readiness (including dissociation)
If you’re a trauma therapist, you already know readiness isn’t a vibe. It’s observable. And it changes over time. Here’s a practical way I think about fit for ART (or any reprocessing model), with dissociation named clearly.
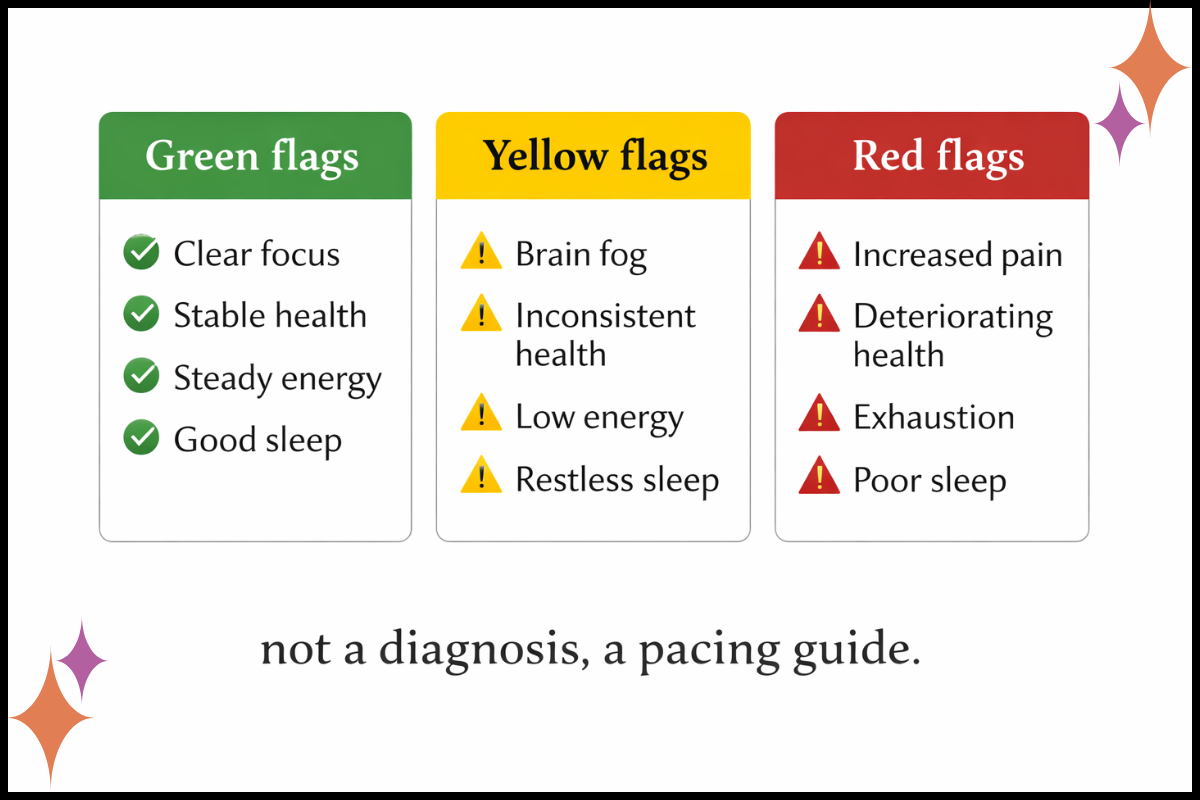
Green flags (often a good match)
A specific memory, image, or trigger that can be named clearly
The person can stay present with activation and come back down
They have some internal skills for grounding or containment (even basic ones)
Their life has enough stability that integration is possible
They want reprocessing work and understand it can be intense at moments
Yellow flags (slow down and plan)
The target keeps shifting and won’t “hold”
High overwhelm or high avoidance that collapses the window quickly
Limited support outside session
High life stress that makes integration harder
Dissociation shows up as spacing out, losing time, going foggy, going numb, or “I can’t feel anything” when you approach the target
Yellow flags aren’t a “no.” They’re a cue to build more structure around safety: more resourcing, shorter sets, more orientation to present time, more explicit consent, and a clear plan for what you’ll do if the client drifts.
Red flags (not “never,” just not first)
Ongoing danger or instability
Severe dissociation without a plan and strong stabilization work
Pressure to “fix it fast” from anyone (including the therapist)
A history of getting worse after reprocessing because pacing wasn’t matched
The client regularly goes out of the window so hard that they can’t track what’s happening in the room
Here’s the dissociation bottom line in plain language: If someone’s system leaves the room when you touch the material, reprocessing is not the first move. The first move is helping them stay present enough that consent is meaningful, pacing is possible, and the work can be integrated.
And if you’re the therapist doing this work: when you’re isolated, it’s easier to confuse “I feel stuck” with “the client needs to move faster.” Consultation protects everyone.
What to ask in an ART consultation
If you’re considering ART for yourself (or helping a client consider it), these questions tend to give real information quickly:
What ART training have you completed, and how often do you use it?
How do you assess readiness for reprocessing work?
What do you do if I get overwhelmed, shut down, or go numb in session?
How do you pace sessions if distress spikes?
Do I have to describe the trauma in detail?
What should I expect after session, and how do you support integration?
What would make you recommend stabilization first?
How do you work with dissociation, shutdown, or losing time?
If you’re a therapist, these questions double as a clean consent framework. Most clients relax when they can feel that you have a plan for safety, not just a plan for technique.
For trauma therapists: using structure without getting rigid
I understand the appeal of structured models. A clear roadmap can reduce drift and help clients feel held.
The risk is when structure turns into rigidity, or when “efficiency” becomes a quiet form of pressure. I don’t want any method to become a way we bypass uncertainty, discomfort, or the slower parts of healing that are actually protective.
If you’re exploring ART, I’d keep two things in your hands at the same time:
Protocols can support effective work.
Your pacing, nervous system tracking, and consultation support are what make that work sustainable.
If you’re craving a place to talk through cases, pacing, and the emotional load of trauma work without performing competence, that’s exactly why I built The BRAVE Trauma Therapist Collective.
Next step
If you take one thing from this post, let it be this: fit and pacing matter as much as the method.
If you’re a therapist, pick one client you’re considering for reprocessing work and ask:
“What would make this slower, safer, and more supported?”
Then get consultation before you push.
If you’re a client, choose two consult questions from above and bring them into the room. You’re allowed to ask for clarity. You’re allowed to ask for pacing. You’re allowed to choose readiness over speed.