
Internal Family Systems (IFS) Therapy: How Parts Work Helps You Understand Your Reactions
What Is Internal Family Systems (IFS) Therapy
IFS is a therapy model that helps clients work with the different “parts” of themselves, including the parts shaped by trauma, protection, and survival. Healing happens by getting to know those parts with compassion, so they don’t have to keep running the show in the same way.
If you’re a therapist, this can be a clarifying model for understanding what’s happening underneath patterns that look like “resistance.”
If you’re a client, this can be the first time therapy language makes your inner world feel understandable instead of shameful.
What “parts” means (and what it doesn’t)
When I say “parts,” I’m not talking about something rare or extreme. I’m naming something most humans recognize the minute they slow down and notice their internal experience.
A part of you wants to go to bed early, and a part of you wants to scroll.
A part of you wants to speak up, and a part of you wants to disappear.
A part of you feels confident, and a part of you suddenly feels like an imposter.
IFS gives us a way to relate to that inner experience without shaming it, flattening it, or pathologizing it.
In IFS, parts are organized around safety and survival. They’re not “bad.” They’re not “the problem.” They’re strategies your system learned.
And trauma (and chronic stress) can make those strategies get rigid.

That rigidity is usually where people get stuck. Protectors can start doing their job the same way they had to back then, even when the danger isn’t current.
So you might notice:
a part that criticizes you constantly because it believes criticism keeps you safe
a part that numbs out because feeling is too much
a part that people-pleases because conflict feels dangerous
a part that works all the time because slowing down makes room for grief, fear, or memory
IFS isn’t about forcing those parts away. It’s about shifting your relationship with them so the system can update.
The key IFS terms people hear and don’t always understand
This is the part I want you to be able to come back to later. These are the words that show up in IFS conversations, trainings, and sessions.
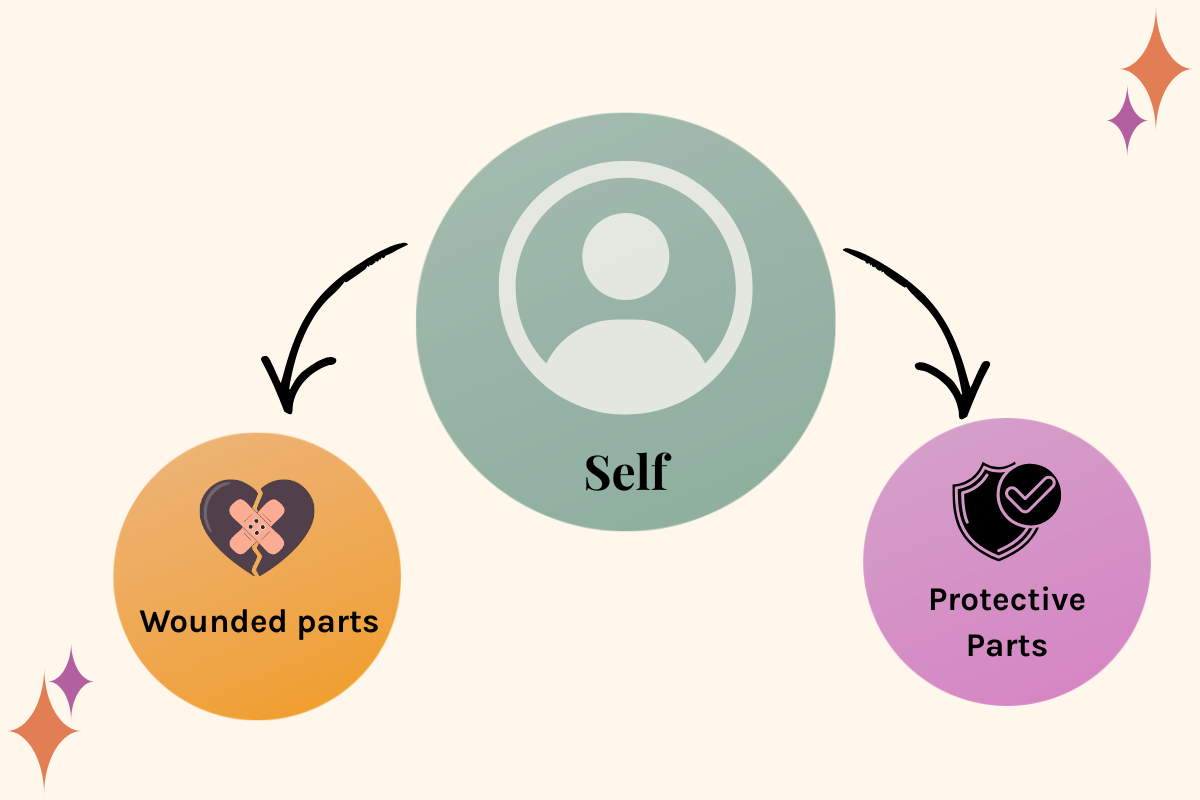
Protective parts
Protective parts are the parts that try to prevent pain from surfacing. They manage. They control. They avoid. They distract. They stay busy. They keep you functioning.
They can look like the inner critic, perfectionism, overworking, caretaking, pleasing, numbing, shutting down, getting angry fast, or staying hyper-logical.
Wounded parts
Wounded parts carry the pain that happened because of stress and trauma: fear, grief, shame, loneliness, helplessness. They’re the places in you that got overwhelmed, didn’t get what you needed, or had to adapt too fast.
In a lot of systems, protective parts are doing their job in relationship to these wounded places. They’re trying to keep them contained.
Self / Self-energy
In IFS, “Self” isn’t a perfect state. It’s not a spiritual performance. It’s more like an internal leadership stance: grounded, curious, calm enough to listen, connected, compassionate, clear.
More Self-energy usually means you can stay with what’s happening inside without getting taken over by it.
Blending
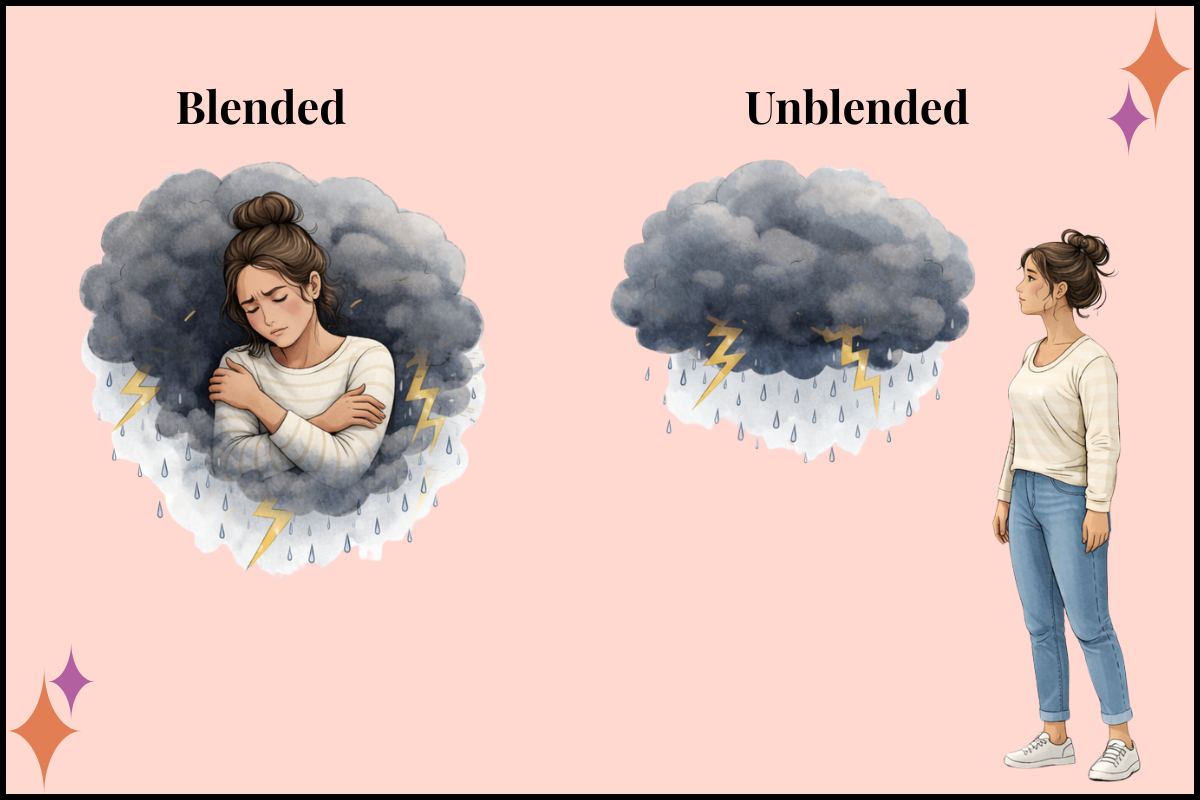
When you’re blended with a part, you don’t experience it as “a part of me.” You experience it as you.
So it’s not “A part of me is terrified.” It’s “I am terrified.”
It’s not “A part of me is criticizing me.” It’s “I’m a failure.”
A lot of IFS work is helping someone create just enough space to relate to a part instead of being fully inside it. That space is where choice becomes possible again.
Where IFS came from and why it’s so integrative
IFS was developed by Richard Schwartz, who noticed that clients naturally described different inner parts with different roles and emotional agendas. Instead of treating that as resistance or dysfunction, he built a model that takes it seriously and works with it directly.
It’s also important to say this: IFS didn’t appear out of nowhere.
There’s a longer history in psychotherapy of working with parts and ego states, and of recognizing that the mind organizes experience into different states, roles, and survival strategies. IFS is one specific model within that longer lineage.
One reason IFS has become so widely used is that it’s integrative. It fits alongside a lot of trauma work that’s already happening.
Here are three ways that shows up clearly:
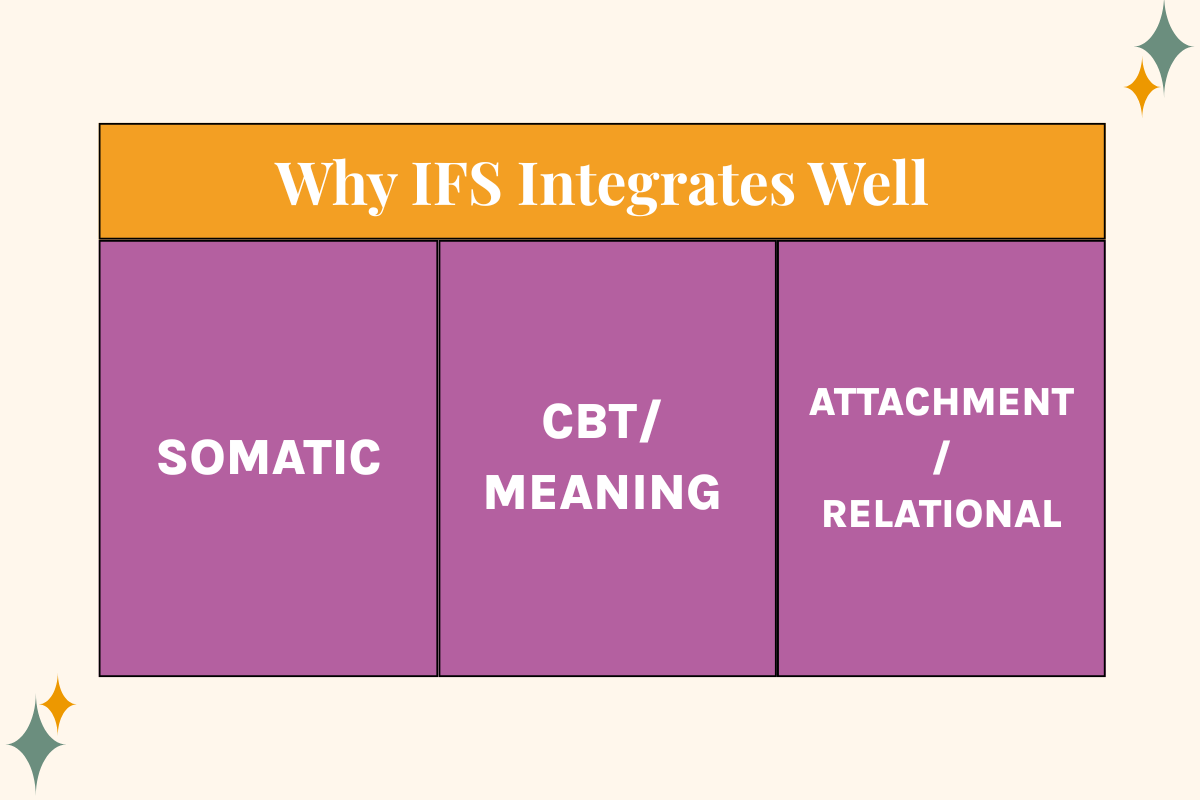
1) Somatic-friendly, even when you’re not calling it “somatic.”
Parts show up in the body. You can track activation, shutdown, tightening, collapse, agitation, numbness. The work isn’t just content and insight. It’s also nervous system shifts in real time.
2) Practical overlap with CBT, without turning it into a debate.
Parts often carry rigid beliefs and meanings: “I’m not safe,” “I’m too much,” “I’m not good enough,” “If I rest, something bad will happen,” “If I say no, I’ll be rejected.”
IFS gives a relational way to work with those meanings that can feel very different than traditional cognitive restructuring.
3) Relational by definition, which is why it fits with attachment work.
Healing isn’t just about knowing why you are the way you are. It’s about experiencing safety in relationship. That includes the external relationship in therapy, and the internal relationship you build with your own experience when you stop relating to yourself with threat and disgust.
What IFS can look like in a real session
This is where people either get it, or they get lost.
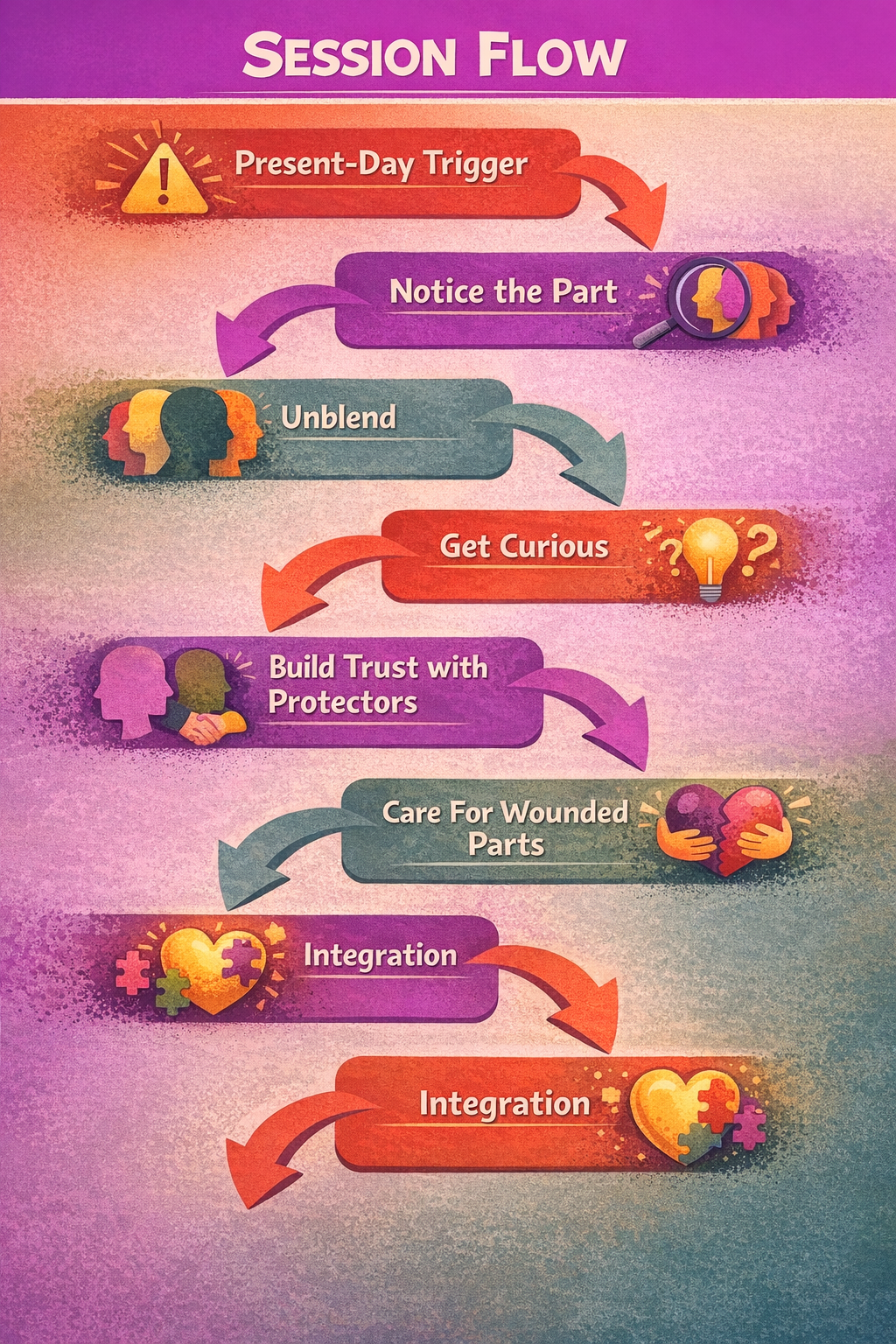
IFS often starts with something present-day:
a trigger, a conflict, a stuck pattern, a shut-down moment, a panic spiral, a behavior you keep repeating.
A trainer I work with regularly likes to begin with:
“What are you most curious about exploring today?”
That question creates space for the system to show itself, without forcing a specific agenda.
From there, instead of trying to fix things from the top down, you get curious about the part that’s present.
You might say:
“My partner and I argued and I got super shut down.”
“I made a mistake at work and totally panicked.”
“I’m exhausted but I can’t stop working.”
Each of those points to a part: the shut-down part, the panicked part, the overworking part that’s trying to prove you’re good enough.
Then the work is slowing down and getting to know the part:
What is it trying to do for you?
What does it fear would happen if it stopped?
What is it protecting you from feeling?
What does it believe is true about the world that makes this strategy feel necessary?
Over time, a lot of clients have the same surprising realization:
the parts they “hate” the most are usually protecting something vulnerable.
And in IFS, you don’t rush past protectors to get to the “real trauma.” You build permission, trust, and stability first.
When the system has enough support, those wounded parts can be witnessed and cared for in a way that wasn’t possible when the trauma originally happened.
You’ll often hear the word unburdening, meaning a wounded part gets to release what it’s been carrying, and the system reorganizes.
Common misconceptions (and why they keep circulating)
IFS gets mischaracterized constantly, and a lot of the critiques come from understandable confusion. Here are the four I hear the most:

Misconception 1: “IFS means I have multiple personalities.”
No. IFS is not saying you have Dissociative Identity Disorder. It’s giving language to internal states, roles, and conflict that many people experience.
And if someone does have significant dissociation, pacing and stabilization matter. IFS can be adapted thoughtfully to work with dissociation rather than against it.
Misconception 2: “Parts work is just imagination / it’s woo.”
Some people use imagery in parts work, but imagery isn’t the same as “made up.” Humans organize experience through sensation, memory, meaning, and metaphor all the time.
If someone says “my chest feels tight,” we don’t call that woo. We call it interoception. Parts language can be another structured way to access what’s already happening inside.
Misconception 3: “IFS is only for complex trauma.”
IFS can be useful for complex trauma, yes. It’s also used for anxiety, depression, relationship patterns, shame cycles, perfectionism, people-pleasing, avoidance, chronic self-criticism, and the experience of feeling like you’re fighting yourself.
Misconception 4: “IFS is about shirking responsibility instead of taking accountability.”
This one matters. Naming parts is not a loophole. In healthy IFS work, naming parts increases responsibility because you notice patterns earlier and have more choice.
Accountability can sound like:
“I understand why this protective part shows up, and I’m still responsible for how I treat people.”
“I can have compassion for where this comes from, and I’m committed to doing it differently.”
A simple parts check-in you can try (client or therapist)
This is not a replacement for therapy, and it’s not meant to turn your day into an internal excavation.
It’s just a short, practical way to build awareness without shame.
Try it once a day, or after a charged moment:
What part of me is up right now? (name it simply: the shut-down part, the proving part, the pleasing part)
What is it trying to do for me?
What does it think it’s preventing?
What do I need right now that isn’t another strategy? (food, water, rest, movement, connection, space)
Sometimes the most important shift is just: “Oh. This is a part. That makes sense.”
A quick word to trauma therapists
IFS asks something specific of the therapist nervous system.
It asks you to be aware of your parts in the room, especially inside the therapeutic relationship. It asks for patience with protectors, consent-based pacing, and the ability to avoid overpowering a client’s internal system with your agenda (or your parts).
Common therapist traps I see:
trying to persuade protectors like you’re arguing them out of existence
moving too fast toward wounded parts because it feels like “the real work”
turning IFS into a script instead of a relationship
performing “Self” like you have to be perfectly calm to do this well
This is one of the reasons consultation and community matter so much in parts-based work. You will get pulled. You will get activated. Your protectors will respond to protectors in your client.
And you shouldn’t have to hold all of that alone.

Inside The BRAVE Trauma Therapist Collective, we focus on sustainability, pacing, and what it means to stay human in trauma work. You’re allowed to take your time. You’re allowed to ask questions. And you’re allowed to stay human while doing this work.
If you’re a trauma therapist looking for support, community, and a place where your humanity is welcome, you can learn more about The BRAVE Trauma Therapist Collective on my website.
And if you’re someone impacted by trauma and wondering whether Cognitive Processing Therapy might be a good fit, you can also visit my website to learn more about my work and reach out if you’re looking for a trauma therapist.