
Which Trauma Treatment Should I Get Trained In?
Which trauma treatment should I get trained in?
This question shows up constantly in therapist spaces. You know, the posts in Facebook groups, consultation forums, and comment threads.
And it can be so risky to even ask this out loud!

Because the moment someone asks, people tend to jump in fast with strong opinions, absolute statements, and proselytizing about the “right” model. Subtle (or not so subtle) messages that if you don’t choose this approach, you’re behind, misinformed, or doing trauma work wrong.
So a lot of therapists stop asking and instead they scroll, they Google, and they quietly panic alone.
If that’s you, I want to be clear from the start: this post is not here to tell you there’s one best trauma model. And it’s not here to convince you to train in what I use.
This is a place to slow the question down.
Why this question feels so high-stakes
This isn’t a casual question.
Trauma trainings are expensive. They take time and emotional energy and they often come at points in your career when you’re already stretched thin.

Underneath Which training should I do? are usually questions like:
What’s actually going to help my clients?
What’s going to sound credible when I name my work?
What if I choose wrong and waste money I don’t have?
What if people take me less seriously?
And there’s another layer we don’t talk about enough: many therapists are trying to make these decisions inside systems that are already overwhelming and under-supportive. There’s very little space to think, reflect, or ask questions without judgment.
So the pressure builds.
The trauma therapy models everyone is talking about
When therapists ask this question, these are usually the models they’re referring to:
EMDR
Cognitive Processing Therapy (CPT)
Prolonged Exposure (PE)
Brainspotting
Accelerated Resolution Therapy (ART)
Internal Family Systems (IFS)
Somatic Experiencing
And even as long as this list is, it is beyond exhaustive. These are currently the most talked-about and most marketed options (share in the comments any I’ve missed!).
Many of them have strong evidence bases and none of them are inherently bad choices but just seeing a list of them, whether here on this blog or in the comments of a Facebook group post, doesn’t actually help you decide.
A more helpful way to think about trauma treatments
Instead of asking which trauma treatment is best, I work with therapists to first understand that trauma interventions exist along a spectrum.
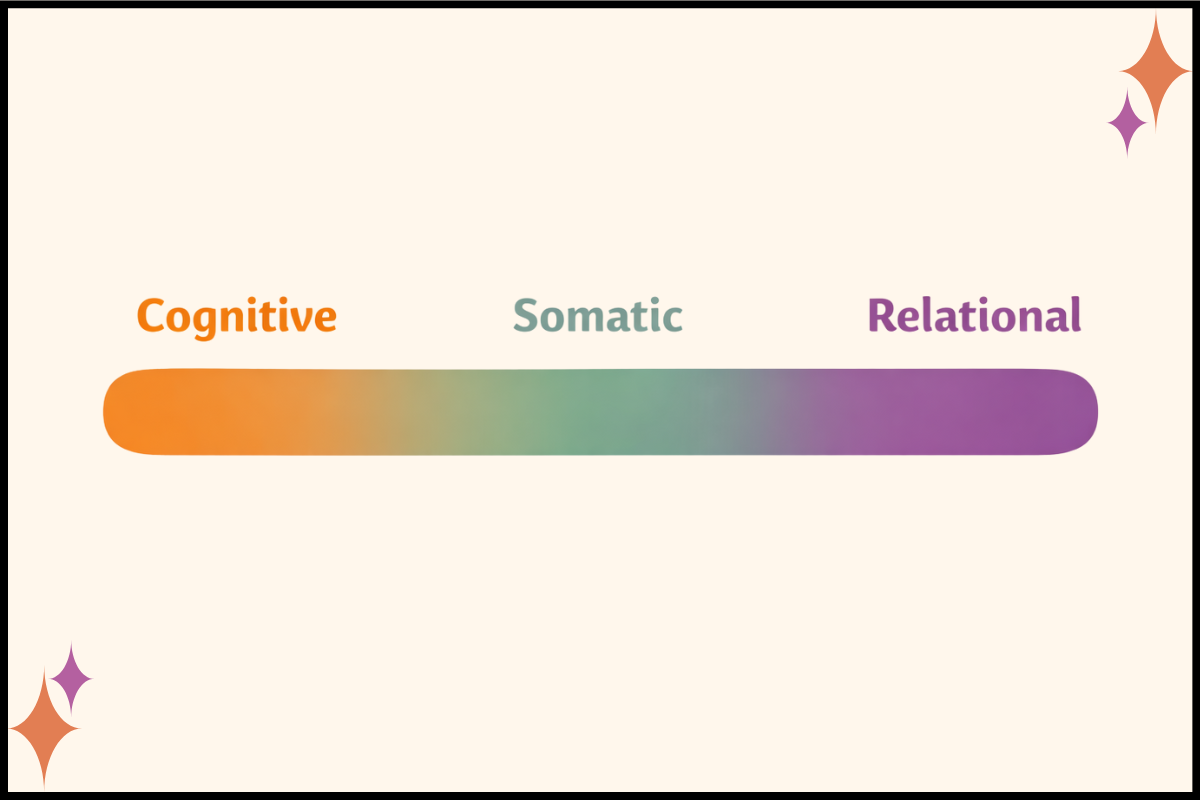
On one end, there are more cognitive and structured approaches.
On the other, more somatic, relational, and parts-oriented approaches.
This isn’t a hierarchy or ranking of which one is best. Rather, these are different containers for this work.
And different clients need different containers at different times just like different therapists thrive in different containers!
Bottom line - fit matters for both effectiveness and sustainability.
How my own training path shaped how I see this
I didn’t set out to collect trauma models or follow trends. I didn’t even realize I wanted to be a trauma therapist way back when - I thought I was going to pursue substance abuse work with teens!
And, as it does, my career unfolded in ways I never could have predicted, and through the work itself.

My early supervision experiences were very psychodynamic and my first formal trauma training was in Trauma Focused-CBT (TF-CBT) and Dialectical Behavioral Therapy (DBT) as I worked with kids affected by child abuse and neglect. Later, I spent years doing highly structured, cognitive work with Cognitive Processing Therapy (CPT) and Prolonged Exposure Therapy (PE) in hospital and academic settings. That work helped clients and it required a lot cognitively and emotionally from me as a therapist.
During the pandemic, I trained in EMDR and worked to bring it into the trauma clinic where I was practicing. That experience brought the relationship back into sharper focus for me, I felt I was returning to a lot of my psychodynamic roots. At the same time, the structure didn’t disappear all while attunement became even more visible in the work.
Later, training in Brainspotting deepened my understanding of somatic processing and naturally introduced parts work. And again, nothing from my past training was abandoned.
Everything integrated.
That’s been the through-line: my training didn’t replace itself, it built on itself.
There are trade-offs, and that’s not a failure
My training experiences, and now my specialty in supporting fellow trauma therapists, has helped me develop this spectrum of training opportunities that ranges from the more structured, cognitive approaches to more somatic.
The more cognitive approaches (e.g. CPT, PE, TF-CBT for kids) can feel grounding and clear. There are clear steps in every single session so you know exactly what to do. At the same time, they can also be cognitively demanding and some therapists and clients might feel they are too rigid.
More somatic and relational approaches (e.g. Brainspotting, Somatic Experiencing, IFS) can deepen presence and flexibility. They can also ask a lot of the therapist’s nervous system and tolerance for uncertainty.
And in between are approaches like EMDR and Accelerated Resolution Therapy (ART), which have very clear protocols but also integrate a lot of somatic and bottom-up work, especially once you’re comfortable with the models.
None of these are better, they’re just different.
And across all of them, one thing stays constant: the therapeutic relationship and attunement matter. No protocol bypasses that and no model replaces that.
What actually helps you choose your next trauma training
Instead of asking Which trauma treatment should I train in? it can help to ask:

Where do I feel most present in session?
What helps me stay regulated when things get intense?
What kind of structure supports me rather than constrains me?
What support do I have while I’m learning?
These questions don’t have flashy answers but when you answer them honestly, they can truly help point you in the right direction.
You don’t have to figure this out alone
These are the kinds of conversations we have all the time inside the BRAVE Trauma Therapist Collective.

We have members who haven’t had access to formal trauma trainings yet. We also have seasoned therapists with multiple certifications who are deciding what, if anything, they want to add next.
What matters isn’t having the “right” answer. It’s having space to think, reflect, and be human while you decide.
A steadier place to land
Training matters in our work. I was just in a meeting with a collaborating partner the other day, talking about how grad school just barely scratches the surface in preparing us to be therapists.
Advanced clinical trainings are necessary, and they’re also protective because when you have the skills to do the work you love, you have greater access to vicarious resilience as you see your clients get better!
But remember this -
No model replaces being human in the room.
No model guarantees confidence or sustainability.
And no model should be chosen under pressure or in isolation.

If you’re feeling stuck with this question, you’re definitely not alone. Reach out! You can contact me any time, and drop your thoughts in the comments so we can all support each other!
And remember, you’re always welcome in BRAVE - you can join for FREE and access our private community plus 1 live call per month or join at just $12 a month and get full access to all our live calls (5+ calls for training and consultation) plus our entire library of past trainings to access any time.
Can’t wait to welcome you!