
The 8 Things That Push Good Therapists Out the Door
You've watched it happen. A therapist on your team, or maybe a colleague you respected, starts pulling back in ways that are hard to name. They're still showing up, still doing the work, still hitting their productivity numbers; but something is different, the energy is different. And then one day, they're gone.
Everyone calls it burnout and maybe that's partially true, but burnout is the last chapter of a much longer story, and the real reasons it was written started accumulating months or even years before anyone noticed.
After years of working with trauma therapists through the BRAVE Trauma Therapist Collective and training organizations on clinician sustainability, I can tell you that when good therapists leave, it's almost never about the paycheck. It's about the slow, compounding weight of working in systems that were never designed to sustain the people doing the hardest clinical work.
Here are eight reasons that weight builds, and why most of them are invisible until it's too late.
Professional Isolation Quietly Erodes Therapist Resilience
Professional isolation is one of the earliest and most corrosive factors in therapist attrition. Trauma therapists carry some of the heaviest clinical material in the mental health field, and most of them carry it without a single peer who truly understands what that's like day after day.

You might have coworkers, and you might even have supervision. But in most settings, supervision stays focused on the case treatment planning, documentation, risk management. All of that is necessary, but it rarely makes space for the therapist themselves. It’s uncommon for someone to ask, “How are you holding up with all of this?” or to normalize the impact that ongoing trauma exposure has on the person doing the work.
When no one is checking on the human behind the clinician, you start to feel invisible in a very specific way. Not invisible as a professional, but invisible as a person. That feeling doesn't show up in week one. It's a slow erosion that builds over months and years until leaving starts to feel like the only form of self-preservation.
And over time, that invisibility reshapes how you see yourself in the work. You stop thinking of yourself as someone whose experience matters, you become the instrument, the intervention delivery system, the clinician who shows up and performs and goes home. The person underneath that role slowly disappears from your own awareness and when you can no longer locate yourself inside the work, leaving doesn't feel like giving up. It feels like the first honest thing you've done in months.
Emotional Invalidation Teaches Therapists to Silence Themselves
"Just leave it at the office." "You knew what you signed up for." "At least you're not the one going through it."
If you've been a trauma therapist for any length of time, you've heard some version of this. Maybe from a supervisor, maybe from a well-meaning friend who has no idea what it actually costs to hold space for someone else's worst moments, over and over again.

And here's what happens when you hear it enough: you stop talking about it. Every time you bring it up, the response tells you that what you're carrying isn't that heavy, or that it shouldn't be, so you go quiet. And when you go quiet, you start internalizing it, you start believing something is wrong with you for struggling; that you should be stronger, more boundaried, more resilient, more something.
That belief doesn't form overnight, it calcifies slowly, one dismissive comment at a time, until the therapist who used to process openly goes silent. And nobody notices, because quiet looks a lot like fine.
And even when a therapist finds a way to push past the invalidation and keep showing up, something else starts quietly compounding underneath the surface.
Administrative Overload Disconnects Therapists from Their Purpose
Administrative overload is one of the most commonly cited reasons therapists leave, and it builds so gradually that most clinicians don’t realize how much it’s shifted until they’re already overwhelmed. What starts as manageable quickly expands into documentation requirements, insurance authorizations, productivity quotas, outcome measures, and compliance trainings that often have little to do with actual clinical practice.
Over time, the ratio of paperwork to client contact keeps shifting, and almost always in the same direction. There’s more documentation, more hoops to jump through, and more time spent justifying the work than actually doing it.
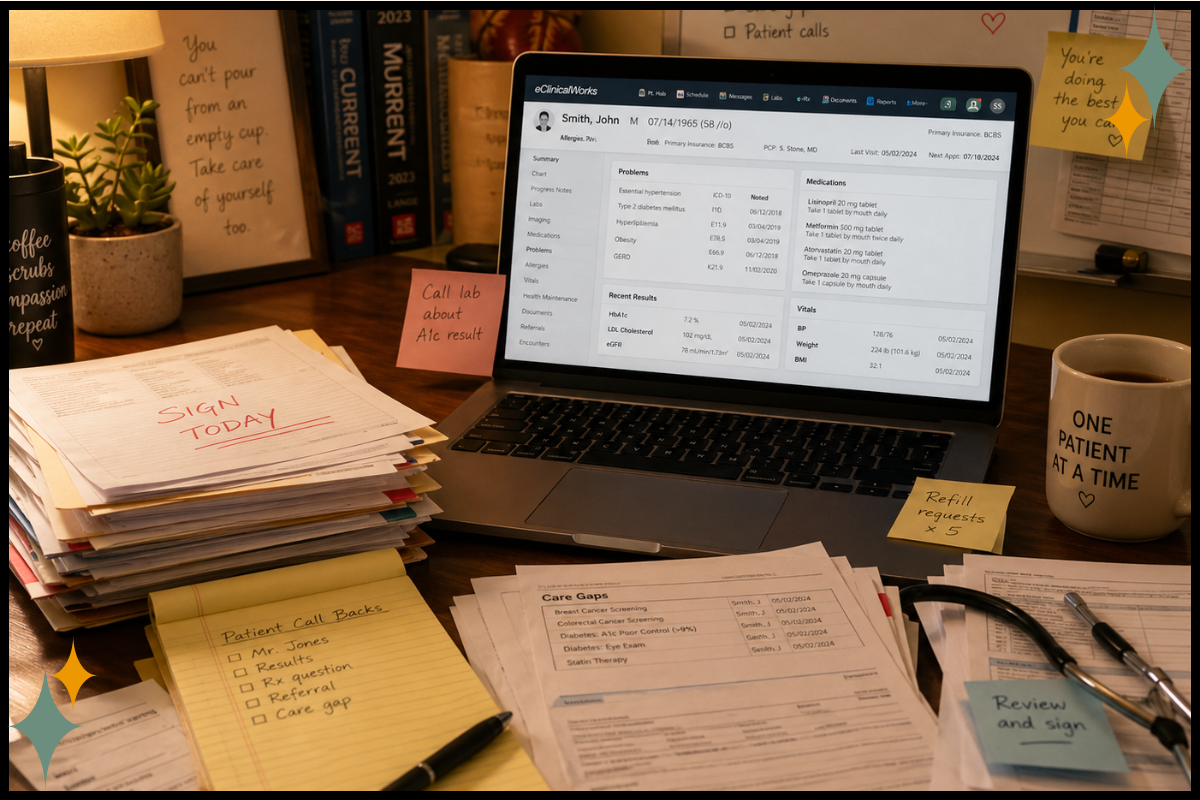
This might feel manageable in the first year, but by year three it becomes deeply draining. Most trauma therapists didn’t enter this field to spend their evenings writing notes; they chose it because they believe in people’s capacity to heal. Over time, every hour spent navigating administrative systems becomes a quiet reminder that the system doesn’t prioritize healing in the same way they do.
What this does to a therapist’s sense of purpose is corrosive in a very specific way. You enter the field feeling called to the work, but that sense of calling slowly gets buried under tasks that have little to do with why you’re here. Eventually, the shift is hard to ignore: you stop feeling like a healer and start feeling like a data entry clerk who happens to hold a trauma therapy license.
The Absence of a Clinical Growth Path Forces Therapists Out of the Work They Love
This one doesn't get talked about enough. In most organizations, the only promotion available to a clinician is moving into management. Becoming a supervisor, a director, an administrator. And all of those roles pull you further from the clinical work that drew you to this field in the first place.

What happens to the therapist who loves being in the room with clients? Who has spent years developing clinical expertise and doesn't want to trade it for spreadsheets and staff meetings? In most settings, they hit a ceiling. There's no advanced clinical track, no role that says, "You can keep doing this work, and we'll honor that with increased responsibility, compensation, and recognition."
When staying in the room with clients is a professional dead end, the most dedicated clinicians start looking for somewhere that values what they actually do, and the organization loses the exact person they could least afford to lose.
But even when a therapist manages to stay connected to their purpose, even when they find ways to navigate the administrative weight and the professional ceiling, there's something else that accumulates in a different register entirely.
Moral Injury Breaks the Connection Between Therapists and the Work They Believe In
Moral injury is different from burnout, and the distinction matters. Burnout is exhaustion, depersonalization, and detachment. Moral injury is a wound. It's what happens when you're trained to provide evidence-based, trauma-informed care and then told you can't, not because you don't know how, but because the system won't let you.
Session limits that cut treatment short just as a client stabilizes, caseload numbers that make quality care impossible, authorization requirements that force you to justify why a trauma survivor needs more than six sessions.
The gap between what you know your client needs and what you're allowed to provide creates a wound that no amount of yoga or deep breathing can heal. No self-care practice fixes the experience of watching a client lose access to care because of a policy decision made by someone who has never sat in a therapy room.
That wound widens with every case where your hands are tied and over time, it changes something fundamental about how a therapist relates to the field itself. You entered this work because you believed in it. Moral injury slowly replaces that belief with something closer to grief. You're not just tired. You're mourning the version of the work you thought you'd get to do.
If you want to start tracking how vicarious trauma and moral injury are accumulating for you, the Vicarious Trauma Tracker is a free tool I created for exactly that.
The Lack of Safe, Honest Clinical Consultation Leaves Therapists Carrying Too Much Alone
This is different from professional isolation. Isolation is about being alone in the work, while this is about not having a space where you can bring your hardest clinical moments without fear of judgment or evaluation.
Most therapists don’t have a single colleague they can be fully honest with about what’s really happening in their clinical work, the cases that scare them, the sessions where they froze, the clients they’re not sure they’re helping, or the moments that leave them quietly questioning whether they’re even good at this.

It’s not that therapists don’t want that kind of space; it’s that most professional environments aren’t actually safe enough to support that level of honesty. Supervision is often evaluative, team meetings can feel performative, and peer consultation, when it exists, can resemble case presentation more than genuine support.
Without a space where they can be fully human about the work, therapists end up carrying everything on their own, and that kind of isolation isn’t sustainable over months, let alone years.
If you're wondering what a genuinely safe consultation space actually looks like, I broke it down in12 Green Flags Your Consultation Group Is Actually Safe.
Surface-Level Wellness Efforts Replace Real Structural Support
Therapists don’t consider leaving because there isn’t a wellness committee; they consider leaving when there is one and nothing actually changes.
If you’re a therapist, you’ve likely seen what this looks like: pizza parties, a one-time training on stress management, or emails reminding you to practice self-care over the weekend. And if you’re a supervisor or leader, you may have offered these in good faith, hoping they would help.
The problem is that, over time, these efforts can send a different message than intended. When clinician wellbeing is treated as a nice-to-have rather than a structural investment, it starts to feel like sustainability is an individual responsibility rather than a shared one.
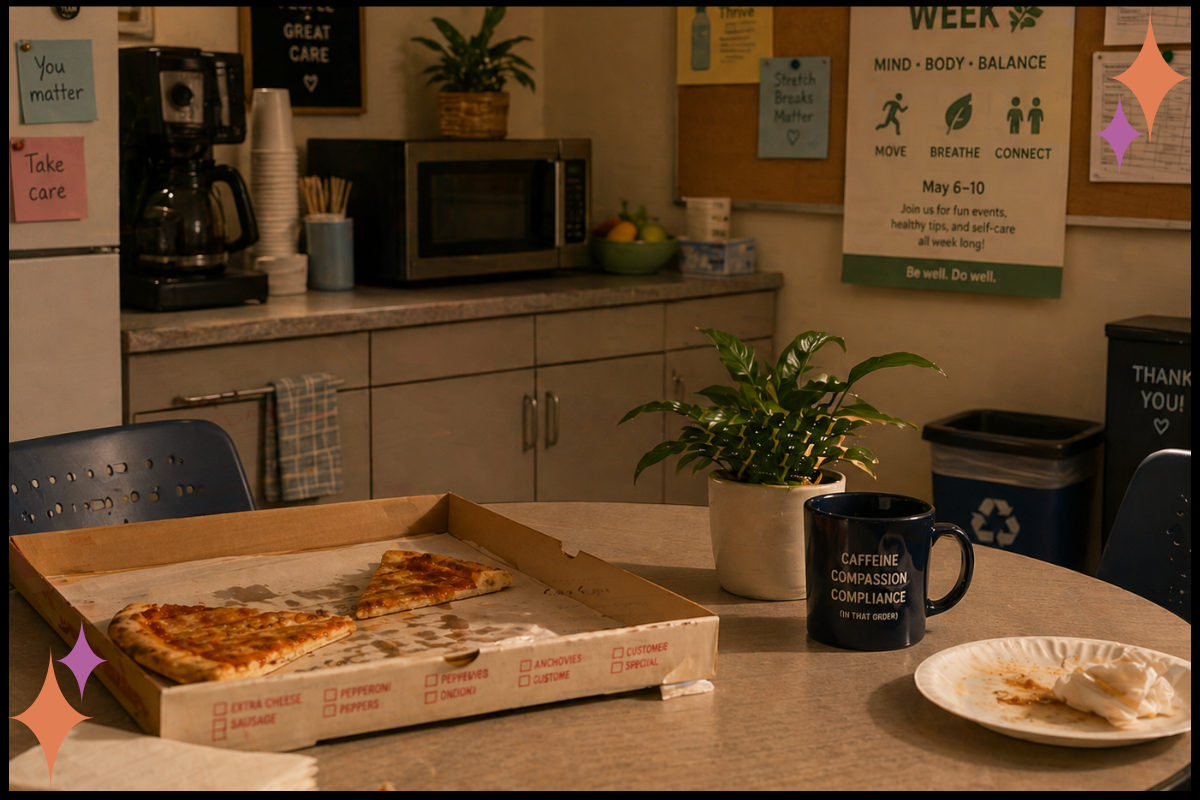
That’s what shifts things. It’s not the absence of wellness programs that pushes therapists toward the door, but the realization that the system they’re working in doesn’t fully understand the difference between a gesture and a real commitment between acknowledging that the work is hard and building structures that actually support the people doing it.
For more on why individual-level solutions fall short, readStop Telling Trauma Therapists to Just Take Time Off.
Organizations Miss the Warning Signs Until It’s Too Late to Retain Their Best Clinicians
By the time a therapist hands in their resignation, the decision was made months ago; sometimes even longer. The signs were there: withdrawal from team interactions, cynicism that used to be humor, quiet disengagement from things they once cared about, the clinician who always volunteered for the hardest cases suddenly going silent in staffings.

But no one had a framework for catching it early, no one was trained to look for it. The organization only notices when the resignation letter lands, and by then, the therapist has already grieved the leaving and moved on emotionally.
The conversation that could have happened eighteen months ago is no longer available.
Every single reason in this article is visible, if someone knows where to look and is actually paying attention. The slow creep is slow, but it is not invisible. What’s missing is not awareness, but systems built to notice it early, before it reaches the final chapter.
These Are Systems Problems, Not Individual Failures
Burnout is the final chapter, but these eight factors are the story that leads there, and most of them have been building for far longer than anyone realized. The therapist didn't just burn out one day. The conditions were set, sometimes years in advance, by systems and cultures and leadership decisions that no one thought to examine.
Every one of these is changeable. Not by the individual therapist trying harder, pushing through, or finding a better morning routine, but by the systems and leaders around them choosing to do something different. Choosing to look at the infrastructure instead of the individual.
Trauma therapists were never meant to carry this work alone, and they shouldn't have to leave it just to survive it.

If you're a clinical director, practice owner, or organizational leader recognizing your team in what you just read, this is exactly what I train on. I work with trauma-exposed organizations to build sustainable consultation structures, leadership frameworks that account for vicarious trauma, and systems that catch the slow creep before it becomes a resignation.Learn more about organizational training.
If you're a trauma therapist who read this and thought, "I wish my leadership understood this," you can send them this article. Sometimes the conversation starts with someone else's words.
And if you're looking for a community where you don't have to carry the work alone, that's why I created the BRAVE Trauma Therapist Collective. It's where trauma therapists come to be human together so they can stay in the work they love.